
Dear Readers,
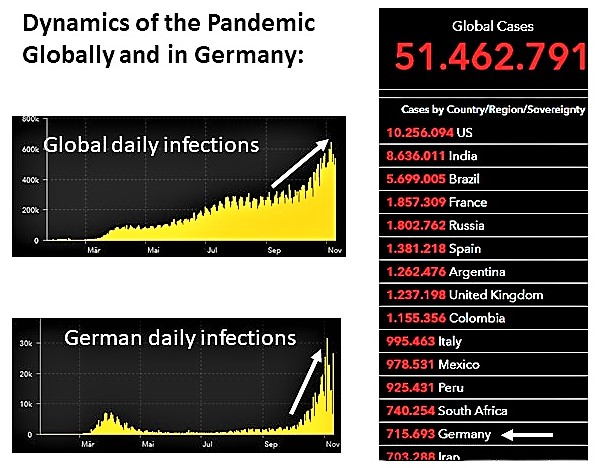
Globally, on October 28, 2020, 44 million people had been infected with SARS-CoV-2, with daily new infections amounting to 500 000, and 1.2 million deaths.
Today, on November 11, 2020, exactly two weeks later, there are 51.5 million infected worldwide, and 1.3 million deaths.
Germany is climbing the table of the Johns Hopkins University, reaching 14th place as if it were a race! Today, we have 716 000 infections. Pandemic development globally and in Germany:
Below we are showing the weekly development, which is growing constantly. Data are from the Johns Hopkins University, which we can understand.
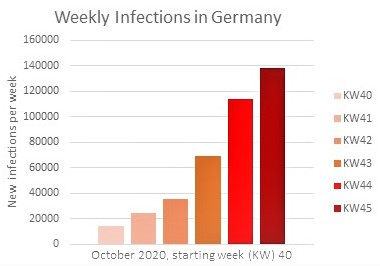
Infection numbers are increasing steadily. We do hope that with a delay of 14 days this trend will flatten. This is depending on each individual’s behavior, and on the accepted, abstained, personal contacts/meetings.

News #1: A possible vaccine may be in sight!
Very good news and a boost of hope was given this week from BioNTech and Pfizer. The press release is making waves, and many scientists are enthusiastic.
However, this is just an intermediate result, the study is not finished yet.
Here is our comment: The control group does not yet show a number of infections high enough to confirm a result. Each experiment is depending on controls. This is true for clinical trials as well.
These data are not available yet. As soon as they are published, we shall have a close look. Until then, we cannot give a scientifically sound evaluation.
The RNA vaccine trial’s cohort is a relatively small number of 40 000.
Questions remain to be answered, such as how many severe COVID-19 cases might have been avoided, or if the vaccine is prohibiting a viral spread from the infected vaccinees.
The population is a mixed one in many respects (age, risk groups…). Only after the study is finished and the final results are published, we shall see what groups may profit most of the vaccine.
A working vaccine would be THE solution to the pandemic. Everybody is hoping this and some more of the 200+ further vaccine candidates will be a success.
The preliminary success announcement of an mRNA vaccine again raises the question on the duration of vaccine-mediated protection from disease. Very recently, two more studies have been published that indicate a decline of SARS-CoV-2 specific antibodies with time. Depending on the initial strength of the immune response, in some individuals, antibodies were detectable after 3 months. In others, however, no antibodies could be found after this time. That means, a vaccine needs to induce a strong response in order to keep the antibody levels high enough for protection over a longer period. This will be one benchmark for the success of a vaccine campaign. At this time this is unpredictable.
https://www.medrxiv.org/content/10.1101/2020.08.05.20169128v1
https://www.nature.com/articles/s41564-020-00813-8
Hint: It may be useful to develop medications based on new molecules.
Each of us knows penicillin or broad band antibiotics that have saved many children and adults. We do have the opportunity to find or develop new broadly acting antivirals.
Wouldn’t you like to have an arsenal of new drugs in the fight against this and future pandemics? For acute phase therapy, for prophylaxis, for the future.
SAJO is making it happen. We are capable to do that. We have our battery of USPs. Please use it. Our appeal to governments: Prepare for the future, it starts tomorrow. Get prepared for further pandemics, with our new molecules, which will be ready in an instant without longer developmental time frames.
Pandemics will become a bigger problem in the course of climate change which is speeding up this development.
News #2: The spread of SARS-CoV-2
On November 5, the Süddeutsche Zeitung mentioned a new study of the Ludwig-Maximilians-Univerity Munich, which we want to comment on:
The study is reflecting the situation in spring.
Antibodies are providing indirect evidence of a previous infection. This, a Munich study used to find out how many people had been infected with SARS-CoV-2 in the spring wave. 1.8 % of the Munich population had been infected, a number four times higher than reported originally. From their data, the authors also concluded the infection fatality rate of 0.76 %. This is a multitude of the one in influenza, to which SARS-CoV-2 is still being compared by those trying to trivialize the situation.
Upon an infection, the virus was able to spread in the household as well as in its proximity up to a distance of 600 ft. Infections are happening in the social context. And: Neither age nor gender or even respiratory allergies seemed to have an impact on severity of disease.
LMU study to COVID-19 in Munich, spring time: http://www.klinikum.uni-muenchen.de/Abteilung-fuer-Infektions-und-Tropenmedizin/download/de/KoCo191/Zusammenfassung_KoCo19_Epi_dt_041120.pdf
SZ article about the results: https://www.sueddeutsche.de/muenchen/muenchen-corona-antikoerper-studie-dunkelziffer-1.5105619
https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-09164-9
Yet another cohort study from Bavaria did show a six-fold higher infection rate in children than previously calculated. This is showing that many more children are getting infected than suggested originally. https://doi.org/10.1016/j.medj.2020.10.003
All these observations are showing that this virus is not to be underestimated. Even the prospect of a vaccine must not lead to a fading of attention. The virus will be a danger for a long time.
Conclusion:
An important point is the fact that in spring, only 1.8 % of the Munich population had been infected.
Even if this number is doubling or tripling in fall/winter, in 2021 there will still be more than 90 % of the population, who are susceptible to SARS-CoV-2.
Once a vaccine is ready (the EU has pre-ordered several hundred million doses), Germany as of today, will receive 18 million doses, so next year there might be 9 million people receiving the vaccine.
Together with those already infected, this is a maximum of 20 % of the population who have at least a partial protection. At max! This is not enough for a general protection of the population. This will be more problematic with the current observations that the antibody-mediated protection is of limited time.
Thus, the current situation will drag on next year. All measures will have to stay in place. As infectious disease experts, we suggest you adjust to these circumstances, on a voluntary basis. That way, the individual risk of infection may be reduced significantly.
Gatherings and meetings should continue to be canceled and replaced by digital events where possible. The spread of this highly contagious pathogen in apartment buildings is posing a – now proven – risk factor. SARS-CoV-2 is an epidemic, highly contagious and underestimated at first. The circumstances and the problems won’t change in the near future. A vaccine will not provide a panacea.
Please get ready to accept that the circumstances – be they accepted by the local governments or not – will not change.
News #3: SARS-CoV-2 is damaging the heart
Very early in the pandemic, it was observed that SARS-CoV-2 not only affects the respiratory tract but is also damaging other organs. At first it was unclear if the virus itself or an immune system going rampant was responsible.
Now it was shown that in addition to immune-mediated damage, the virus itself may inflict harm on the heart muscle. Two new studies made this clear. One team examined a case of a young mother who had mild COVID-19 symptoms, but suddenly died of heart failure. SARS-CoV-2 was detected in the heart tissue, and it was shown that the viral spike protein alone was inducing fusions of cardiomyocytes, which resulted in a massive damage of the heart muscle. A second team proved that SARS-CoV-2 could indeed infect heart muscle cells. These cells are carrying the ACE-2 receptor the virus needs for an infection. Infection of these cells triggered a myocarditis resulting in a severe reduction of contractility.
https://www.researchsquare.com/article/rs-95587/v1
https://www.biorxiv.org/content/10.1101/2020.11.04.364315v1
These two works are showing that this virus is highly dangerous and may be deadly for younger people as well.
Appeal to all of you: For everybody and everyone at any place of the world: Do as good as you can!
We advocate the AHACL (the typical German abbreviation, non-translatable), reminding on the Aztec god: The AHACL (in some circles also referred to as the Merkulix rules) mean: Distance, hygiene, face mask, virus app, and ventilation.
More elaborately (we will repeat until it is memorized) – The Merkulix-formula “The AHACL”:
Keep a physical distance! 2 meters / 6 feet!
Wash your hands regularly and thoroughly!
We recommend medical N95 face masks, also for visits in the doctor’s office, in every setting where a distance may not be possible.
Keep making visits in the outdoors even now. There are warm clothes, and fresh air does not hurt. Even better: Cold temperatures activate sirtuins in the cells, which act against cellular ageing.
Make sure, regular ventilation is achieved in indoor settings with several people.
Please reduce your mobility, your in-person-contacts to a minimum, and avoid unnecessary travel. Parties of every kind currently are not acceptable. They not only pose a risk, they also indicate a severe lack of respect of the pain this virus is inducing.
Out-door sports are ok, with individual distance.
At the moment, it is most important to get through winter as good as possible, to keep damage to people and economics as low as possible. Please, do your part.
Stay alert and healthy!
Yours, Sabine and Jörg

SAJO is consulting all around infectious diseases. We are applying our know-how, that we have acquired in more than 20 years. We do what we can to fight this pandemic.
SAJO – for a healthy world and better future!
To our delight our blog is receiving a lot of acceptance, we love to share our knowledge. Single posts and contents are being adopted by others, also in media. We have learned how to correctly make a citation; this we would wish from others in return as well. Please feel free to share the link.
If you like our blog and do find it helpful, please feel free to support the blog: SAJO, IBAN: DE19 7016 9464 0000 5444 50, BIC: GENODEF1M07, Re: sajo blog
Your contribution will provide support for our colleagues who are working behind the scenes of the blog. Sabine and Jörg continue to work on this pro bono.
If you want to award a contract to SAJO, or if you want to have us consult you, please get in touch.
Would you like to have SAJO antivirals and/or antibacterials?
If you want to support drug development, please feel free to contribute as much as you feel happy to: SAJO, IBAN: DE19 7016 9464 0000 5444 50, BIC: GENODEF1M07, Re: sajo drug development
The amount will be used for SAJO drug development.
Note: The company SAJO up to now has been funded by private means by Sabine and Jörg. More than € 500,000 were put into the development of the SAJO key technology. To take the next step, to develop SAJO drugs – antivirals and antibacterials – we are asking for R&D contracts and support.

